I don't like predictions or reviews, but it seems bloggers are obliged to do this. I did make predictions last year, so I must also measure myself against those predictions.
I am still excited by opportunities and results.
 |
| Speed Bump Comic Strip |
Less Blog posts in 2013 and 2014
My job at GE Healthcare is to create and promote Interoperability Standards; specifically in HIE, Security, and Privacy. This means that I have a dual focus: outside development in standards organizations (HL7, DICOM, IHE, ISO) and government adoption (S&I Framework, HIT-Standards, HealtheWay, WISHIN, epSOS, Saudi-MoH); and inside promulgation of those standards into products and services. The outside efforts had been put into place in the previous years, and had a reasonable trajectory; so my focus this year has been far more internal focused. Thus I have created less blog articles in 2013. In the three previous years I have created about 95-97 articles, with some months producing 14 or more (thanks to ONC). In 2013, I have only produced 56 articles, with one month with 12 articles (thanks to HL7 ballots including Digital Signatures, DS4P, and FHIR). Some people try to produce a blog article every day, I am happy with one a week, or one a month.Past Predictions
I predicted three themes for 2013: Mobile, Privacy, and Services. The following themes that appeared throughout the year nicely fit these three high level themes, most of the time fitting all three (Accounting of Disclosures).
Measurements toward Predicted Theme
The themes that appear in 2013 posts
- mHealth Security (1), (2), (3), (4), (5), (6), (7), (8), (9), (10), (11), (12)
- FHIR (1), (2), (3), (4), (5), (6), (7), (8)
- Safety (1), (2), (3),
- Privacy (1), (2), (3),
- DS4P (1), (2), (3),
- De-Identification (1), (2), (3),
- Accounting of Disclosures (1), (2), (3), (4),
- HIE (1), (2), (3), (4), (5), (6), (7), (8),
- Digital Signatures (1), (2)
This is satisfying to me, but not what my blog Google Analytics show was most interesting to the readers during 2013. The top most viewed articles are all from 2011 and 2012. One of them I didn’t even write.. In order, the most popular Posts in 2013 by click count:
- Meaningful Use Stage 2 - Audit Logging - Privacy and Security
- Meaningful Use Stage 2 -- 170.202 Transport
- How to apply Risk Assessment to get your Security and Privacy and Security requirements
- IHE - Privacy and Security Profiles - Audit Trail and Node Authentication
- Creating and using Unique ID - UUID - OID
- Topics (my table of contents)
- Patient Portal - view, download, TRANSMIT
- IHE - Privacy and Security Profiles - Basic Patient Privacy Consents
- How granular does an EHR Security Audit Log need to be?
- The Basics of Cross-Community Patient Discovery (XCPD) - Guest blog by Karen Witting
Posts fading away
I was glad to see these past popular articles become less interesting. They are all now 3+ years old, and likely not accurate today. Please let them fade away.- Meaningful Use Encryption - passing the tests
- Meaningful Use Certification issue with Encryption of data-at-rest
- Meaningful Use Security Capabilities for Engineers
I am very happy that the most top viewed article posted in 2013 during 2013 was the one where I Define Privacy. This comes in at the 15th most popular article this year. The other articles written in 2013 that breaks the top 40 are where I Define Security Audit, and try to Define mHealth. Is this telling me that I should be in the Definition or Vocabulary space? I also posted this year that Vocabulary Standards make poor User Interfaces.
Predicting 2014
I suspect that the US government will continue to be consumed by things that are already in play. There will be a small number, mostly ONC and HIT committees, that keep trying to figure out what MU3 should be. The problem they will face is that it is not clear what the benefit of MU3 is going to be when so many are consumed by things already in play.
Bluebutton+ will seem right, yet confuse. There will be some easy things, like "Bluebutton+", but as I point out on Keith's blog this is too nebulous of a specification to figure out what it means. The message needs to be made more clear, what part of the "Bluebutton+" experience is to be mandated and measured? I hope it is the CCDA, and not the transport. But Keith sees it otherwise.
I don't object to the transport but it is pre-standards specification. I would rather see us mature the "RESTful" concept under FHIR and MHD, with security models from IUA, DS4P, and other projects underway. Getting this right is more important than getting it done fast. This is not to say that HIEs should not look to Bluebutton+, they should. The action should be to experiment and reflect on that lessons learned so that we improve the standards so that we get something worthy of mandate and measurement.
HIE Patient Identity. We will continue to work on the Patient Identity problem, more so this year. There was much talk in the past few years. There was some intense, urgent, work done in CCC and CommonWell. This work will be brought out into the open. We will learn that this is NOT at technical problem, the standards support what is needed. This is a 'business' operational issue, and a 'privacy' issue. Meaning businesses don't want to change what they are gathering, yet everyone gathers different information. If we must do patient matching, then we must all gather the same demographics with the same level of accuracy (Level of Assurance). For example, everyone must gather the SSN completely, not just the last four digits. This brings up the 'privacy' problem that this creates. We will not see a universal patient ID, but we will see what sure looks like one. It will simply be a well-structured-and-normalized mashup of the demographics all hashed together. This will fail to match sometimes, but it won't have false matches (false-positive).
Profiles. Simply the USA will realize the need for Profiles. This might not be "IHE" profiles universally. I am okay with that. I fully expect that HL7-FHIR will produce some profiles this year. I fully expect that HHS/ONC/HIT-Sc/HIT-Pol/S&I-Framework will come up with a concept closer to a 'profile'. This is not far off, but not being done today with purpose. The purpose will come when the community sees what IHE does with DS4P. The result is simple and measurable.
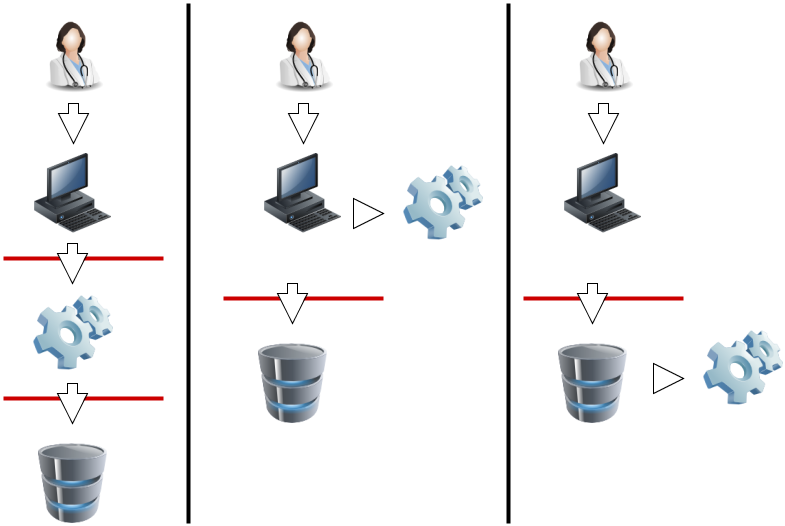
 |
| Add caption |
HIE Patient Identity. We will continue to work on the Patient Identity problem, more so this year. There was much talk in the past few years. There was some intense, urgent, work done in CCC and CommonWell. This work will be brought out into the open. We will learn that this is NOT at technical problem, the standards support what is needed. This is a 'business' operational issue, and a 'privacy' issue. Meaning businesses don't want to change what they are gathering, yet everyone gathers different information. If we must do patient matching, then we must all gather the same demographics with the same level of accuracy (Level of Assurance). For example, everyone must gather the SSN completely, not just the last four digits. This brings up the 'privacy' problem that this creates. We will not see a universal patient ID, but we will see what sure looks like one. It will simply be a well-structured-and-normalized mashup of the demographics all hashed together. This will fail to match sometimes, but it won't have false matches (false-positive).
Profiles. Simply the USA will realize the need for Profiles. This might not be "IHE" profiles universally. I am okay with that. I fully expect that HL7-FHIR will produce some profiles this year. I fully expect that HHS/ONC/HIT-Sc/HIT-Pol/S&I-Framework will come up with a concept closer to a 'profile'. This is not far off, but not being done today with purpose. The purpose will come when the community sees what IHE does with DS4P. The result is simple and measurable.
And everything else. Yes Security, Privacy, and HIE will continue to evolve and mature. This is going along at the right pace. Many want it faster, but faster is not how one moves such a large industry like healthcare. Especially since healthcare is very much thousands of competing organizations with highly educated and driven individuals as the workers. My themes from last year will continue to be the right themes: Mobile, Safety, and Services.
Optimism
Overall I am excited at our progress. It really is a team-sport. There are far more people 'doing' than ever before. There is a more common goal than ever in the past, and the majority of efforts are all clearly toward that goal.